The first thing I look at on a neck isn’t the skin.
If your neck looks full and your jawline soft — and you’re not overweight, or you’ve lost the weight and it’s still there — you’ve probably been told it’s fat, loose skin, or just aging. Often it is. But sometimes the real reason is something no diet, no filler, and sometimes not even a facelift can fully change on its own: the position of a small bone in your neck called the hyoid.
When a patient sits down to talk about a facelift or a deep neck lift, the first thing I assess isn’t the skin — it’s where the hyoid sits, because it quietly sets the ceiling for how sharp your neckline can ever become. Understanding it is one of the most honest things I can share in a consultation.

What the hyoid bone actually is
The hyoid is unusual. Unlike nearly every other bone in the body, it doesn’t lock into a joint with another bone. Instead, it floats — suspended by a sling of muscles and fascia that connect your tongue, jaw, and voice box. [3]
Functionally, it’s essential to swallowing and speech. Aesthetically, its vertical and front-to-back position helps set the cervicomental angle — the angle between the underside of the chin and the front of the neck. That angle, more than almost anything else, is what your eye reads as a “young,” defined neck. [1]
Why hyoid position can make or break a neckline
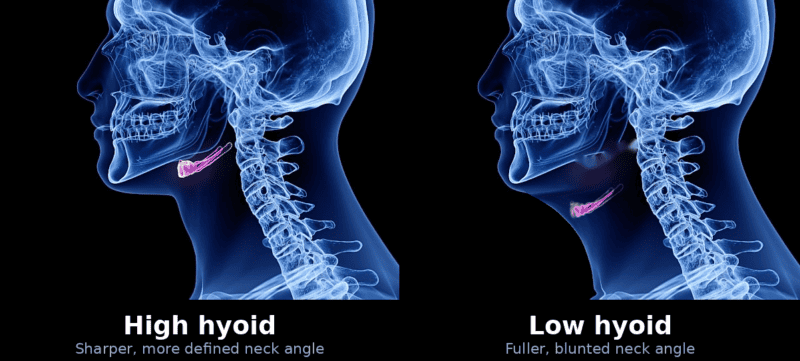
A higher, more tucked-back hyoid tends to give a naturally sharper cervicomental angle and a more sculpted neck — often one that ages gracefully. [1]
A lower or more forward hyoid does the opposite. It predisposes to a blunted, more open neck angle and a “heavier” look — even in a patient who is otherwise an excellent candidate and not carrying extra weight. I want to be clear about something: that is an anatomic starting point, not a surgical failure, and it is not something weight loss alone will correct. [1,2]
When the hyoid sits low or forward, I commonly see:
- A more obtuse (open) cervicomental angle
- Less jawline definition
- A neck that looks shorter, or fullness under the chin that lingers no matter what
This isn’t just my observation. In a cadaveric study of neck-contouring techniques, a low hyoid was the only preoperative factor that significantly limited how much the cervicomental angle could be improved — a direct demonstration of how this one variable can shape, and sometimes cap, the result. [5]
A real example from my practice — the same surgery can yield different necklines depending on where the hyoid starts:

Consented patient. Profile before/after showing a sharp, well-defined neck angle (favorable high hyoid).

Consented patient. Profile before/after showing the fuller result a low hyoid imposes even after deep neck work.
What a deep neck lift can — and can’t — change
A deep neck lift goes well beyond tightening skin. In the right patient it addresses the deeper drivers of an aging or full neck: the platysma muscle, the fat beneath it (subplatysmal fat), the anterior belly of the digastric muscles, and in some cases prominent submandibular glands. [3]
But I’m always honest about the limit: even the most complete deep neck lift doesn’t change who you are anatomically. I don’t routinely reposition the hyoid bone itself, and its baseline position remains a foundational determinant of your final neck angle. [1] What surgery can do is optimize everything around it — reducing deep fullness, refining the muscle layer, and managing the fascial planes — to deliver the best contour possible within your structural framework. [2,3]
How I address a low hyoid surgically
In a patient with a low hyoid, I can’t move the bone — but I can soften its influence by addressing the muscles that tether it, and I do this routinely in these cases.
The hyoid is held in place by both suprahyoid and infrahyoid muscles that pull down and forward on the larynx and central neck. When I operate on a patient with a low hyoid, I routinely perform a selective release of specific infrahyoid muscles — most often the sternohyoid and omohyoid — to reduce that downward, forward tether on the hyoid–larynx unit. [2,4]
This doesn’t reposition the hyoid in any skeletal sense, and it isn’t something every neck needs. What it does, in the right patient, is ease the downward pull on the central neck so I can open up the cervicomental angle further than soft-tissue work alone would allow — particularly in a low-hyoid patient who otherwise has favorable anatomy. [1,4] Because these muscles contribute to swallowing and voice, the release has to be conservative and precise, which is exactly why it belongs only in the hands of a surgeon who works in this anatomy routinely. [2,3]
Even then, the principle holds: the goal is optimization, not transformation. The result is still bounded by the anatomy you start with — but for a low-hyoid neck, this step is often what makes the difference between a modest improvement and a genuinely sharper, cleaner result.
Working with your anatomy: the deep plane facelift
The deep plane facelift repositions the deeper layers of the face rather than relying on skin tension — which is what produces a natural, durable result instead of a pulled one. [2] Paired with the right neck work, it can sharpen the jawline, restore balance between the face and neck, and create a smoother cervicomental contour.
This is the heart of how I approach facial rejuvenation with the 4D Facelift™ — lift, volume, and skin quality addressed together, and always in step with a patient’s underlying structure. The most refined results happen when technique and anatomy are aligned, never forced. Hyoid position is simply one of the most important “baseline settings” that tells me what’s achievable in the lower face and neck. [1,2]
Why I spend consultation time on this
One of the most valuable parts of a facelift consultation is education. When a patient understands the role of the hyoid, they finally understand why two people can receive the same high-level surgery and get different necks — it isn’t about effort or technique, it’s about where they started.
My preoperative evaluation of the aging face and neck routinely includes:
- Hyoid height and front-to-back position
- Mandibular projection and skeletal support
- The deep central neck — subplatysmal fat, digastric muscles, gland prominence
- Skin quality and elasticity
The peer-reviewed neck-lift literature backs this up: achieving an ideal cervicomental angle is largely governed by the relationship between skeletal support, soft-tissue volume, and hyoid anatomy — and some necks are simply, inherently more difficult because of these variables. [1,2]
The takeaway
Hyoid position is a powerful and underappreciated driver of how a neck looks. It can’t be reliably repositioned, but its influence profoundly shapes what a deep neck lift, deep plane facelift, or full facelift can deliver. [1,2]
Modern facelift surgery is not about pulling skin — or even just tightening the platysma. A refined, natural neck comes from detailed planning, a real understanding of anatomy, and the surgical judgment to work safely in the central neck when it’s appropriate. Approached that way, the result isn’t an operated look. It’s a neck and jawline that simply look balanced, elegant, and timeless.
Ready to talk about your neck?
If your neckline has never looked as sharp as you’d like — or a previous procedure didn’t fully deliver — a large part of the answer may be anatomy you were born with. The right plan starts with an honest evaluation of it. You can also watch my full video on the hyoid and neck contour.
Request a consultation or call 281-557-3223. Dr. Raghu Athré, MD, FACS — double board-certified facial plastic surgeon, Houston, TX.
References
- Fedok FG. The Difficult Neck in Facelifting. Facial Plastic Surgery (2014). https://pubmed.ncbi.nlm.nih.gov/25076452/
- O’Daniel TG. Optimizing Outcomes in Neck Lift Surgery. Aesthetic Surgery Journal (2021). https://pubmed.ncbi.nlm.nih.gov/33543747/
- O’Daniel TG. Understanding Deep Neck Anatomy and Its Clinical Relevance. Clinics in Plastic Surgery (2018). https://pubmed.ncbi.nlm.nih.gov/30268237/
- Le Louarn C. Hyo-neck lift evolution: Neck lift with fixation of the platysma to the deep cervical fascia. Annales de Chirurgie Plastique Esthétique (2017). https://pubmed.ncbi.nlm.nih.gov/29292051/
- Dabb RW et al. A Comparative Study of Surgical Techniques on the Cervicomental Angle in Human Cadavers. Archives of Facial Plastic Surgery (2002). https://pubmed.ncbi.nlm.nih.gov/12437429/