Jowls are one of the most common reasons patients come to see me — but the first thing I do is figure out what a patient actually means by the word, because it’s usually one of two different things.
First: which line are we actually talking about?
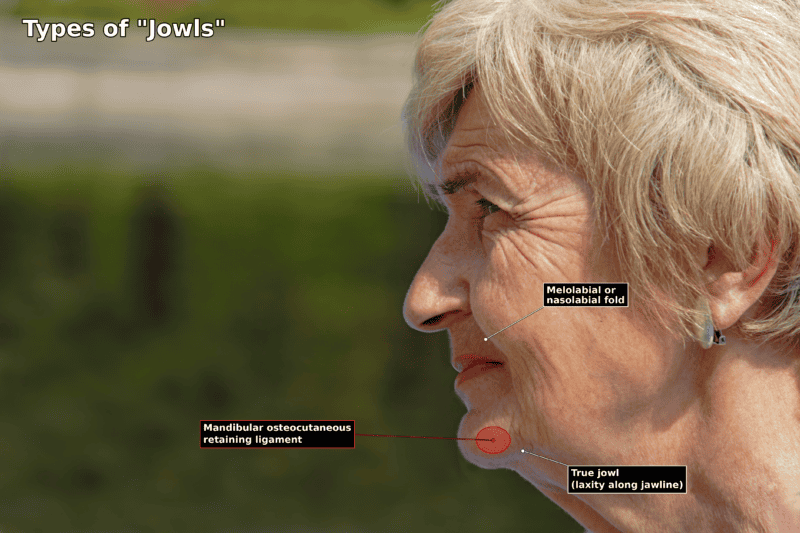
When someone says their jowls bother them, they’re almost always pointing at one of two areas:
- The true jowl — the soft fullness right along the jawline, at the marionette line and the mandibular margin.
- The melolabial fold — the “smile line” running from the nose to the corner of the mouth. Patients frequently lump this in with their jowls, even though it’s a separate structure higher up the face.
This distinction matters, and it has to be made before we talk about any treatment, because the two areas don’t always call for the same thing.
Either way, both are the same kind of problem underneath: a structural line created by soft tissue that has descended and lost its support — but is still tethered down to the deeper face by the retaining ligaments. In my opinion, all of the retaining ligaments of the face share in this tethering as the tissue drops; it’s not solely the work of two of them. That said, the zygomatic and mandibular retaining ligaments are probably responsible for something like 90% of what we see as jowls and melolabial folds, with the masseteric and the others contributing the rest. (I go deeper into these structures in my post on the retaining ligaments of the face.)
So a jowl or a deep smile line is descended structure, held down at fixed points. It is not simply loose skin — and that’s the whole reason skin-only treatments so often disappoint.
Treating it: the answer depends on how far the tissue has dropped
Because these are structural lines, the right treatment scales with how much descent there is.
Mild folds — camouflage with volume
If the melolabial fold or the true jowl is mild, it can often be camouflaged by adding volume — essentially softening the difference between the dip and the fullness around it. Two good options here:
- Fillers — a straightforward, in-office way to blunt an early fold.
- Fat transfer — my personal preference, using your own tissue for a more natural, longer-lasting result.
Be clear about what this category does, though: you’re filling around the line, not lifting the tissue that created it. For early, mild folds that’s often exactly enough. For anything more advanced, it isn’t.
Moderate to severe folds — resuspension (a facelift)
Past a certain amount of descent — once the folds are moderate to severe — volume can’t fix the problem, and you genuinely have to resuspend the tissue. That, in practice, means some form of facelift: repositioning the descended structure back to where it came from rather than resurfacing or filling around it.
If the melolabial fold or the jowl/jawline fold is extremely deep, you need a deep plane approach specifically — disarticulating the retaining ligaments so the tissue is fully released and can be resuspended cleanly along the right vector. Without that ligament release, you can’t get a true, natural correction of a deep fold.
Very mild folds that still need lifting — a less intensive option
Not every fold that needs resuspension needs the full operation. For very mild folds that still require some lifting, you can sometimes get away with a less intensive technique — my Headband Lift™ — and still achieve a good result with a decent amount of longevity and success.
A special case — when the real problem is the chin
There’s one important exception to all of this. Sometimes what looks like a jowl is really being created by a foreshortened or recessed chin. When the chin lacks projection, the jawline loses its frame and the pre-jowl area looks deeper than it otherwise would. In those patients, the answer isn’t a lift at all — it’s rebuilding the foundation with a chin implant, which restores projection and can dramatically improve the jawline and pre-jowl contour. Identifying this case correctly is exactly why the evaluation matters.
The honest part
Here’s what I tell patients, and it isn’t always what they expect: if your jowls or smile lines are early and mild, you may not need surgery — a little filler or fat can carry you a long way. But if those lines are established, be wary of anyone promising to “lift” them with injectables or energy devices. Those treat the surface. These lines are descended, tethered structure — and correcting them means releasing and resuspending that structure, or, in the right patient, rebuilding the chin underneath it.
Figure out which one you’re dealing with
The fastest way to stop guessing is an evaluation that looks at your actual anatomy — which line is involved, how far it’s descended, and whether your chin is part of the picture — instead of a one-size-fits-all menu. That’s the aging face and neck consult I do every day.
Request a consultation or call 281-557-3223.
References
- Furnas DW. The retaining ligaments of the cheek. Plastic and Reconstructive Surgery (1989);83(1):11–16.
- Rossell-Perry P, Paredes-Leandro P. Anatomic Study of the Retaining Ligaments of the Face and Applications for Facial Rejuvenation. Aesthetic Plastic Surgery (2013). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3657075/
- Mendelson BC, Wong CH. Surgical anatomy of the middle premasseter space and its application in sub-SMAS facelift surgery. Plastic and Reconstructive Surgery (2013). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3636554/